
Written by: Crystal Maertens
This article covers a topic that is part of Champ Software’s Expert Webinar series, in which subject matter experts present on trending or urgent public health topics. Join our mailing list here to receive expert webinar invitations.
In February 2021, Tanya Carter presented at one of Champ Software’s expert webinars, providing an overview of comprehensive suicide prevention.
Tanya Carter is the Suicide Prevention Supervisor at the Minnesota Department of Health, with over 20 years of experience in community education program development and crisis intervention. She is passionate about suicide prevention and reducing the stigma related to mental illness.
Her presentation described how the Minnesota Department of Health’s Community Partners Preventing Suicide (CPPS) program is working with Minnesota partners to implement suicide prevention in selected communities. CPPS uses a comprehensive public health approach to build capacity within systems and organizations. The strategies, tools, and best practices used are flexible and culturally appropriate to address and plan for suicide prevention in communities. Tanya’s presentation focused on all levels of partnerships and suicide prevention being implemented: the Zero Suicide Framework, school-specific comprehensive suicide prevention planning, community readiness assessment, and strategic planning.
Introduction:
Carter began her presentation by acknowledging the emotional nature of the topic: “Suicide is a devastating loss. We’ve all been touched by a loss at some point in our lives. And if you’re a survivor grieving a suicide, know that you’re not alone.” She also urged anyone struggling with painful emotional memories as a result of the presentation to care for themselves and seek support from family, a friend, or the national Suicide & Crisis Lifeline which, as of 2022, can be reached by dialing 988. From the 988 Lifeline website: “The 988 Lifeline is a national network of local crisis centers that provides free and confidential emotional support to people in suicidal crisis or emotional distress 24 hours a day, 7 days a week in the United States.” [1]
Causes of Suicidal Behavior
“What causes suicidal behavior?” Carter asked, “You know that’s a really great question, right? Suicide is complex. There is not one single path that can fully predict or explain what leads to suicide. Suicide most often occurs when stressors and health issues converge to create an experience of hopelessness and despair.”
Carter noted that depression, which is often undiagnosed or untreated, is the most common condition associated with suicide. “Conditions like depression, anxiety, and substance problems, especially when unaddressed, increase our risk for suicide. Yet, it’s important to note that most people who actively manage their mental health conditions go on to engage in normal life.”
Carter listed several factors that could increase the risk of suicide as well as several that could protect against it: “… and each of those factors has complicated relationships with suicide and, in fact, with each other.”
Risk Factors for Suicide
Carter’s slide for this portion of her presentation described a risk factor as “a characteristic at the biological, psychological, family, community, or cultural level that precedes and is associated with a higher likelihood of suicidal outcomes.”
Examples of risk factors that Carter listed included:
- Substance use
- Mental health conditions (e.g., depression, bipolar disorder, schizophrenia, conduct disorder, or anxiety)
- Serious physical health conditions
- Environmental factors such as access to lethal means (e.g., firearms, drugs, etc.)
- Prolonged stress (e.g., harassment or bullying)
- Relationship problems
- Loss of a relationship, job, finances, etc.
- Stressful life events (e.g., divorce, financial crisis, etc.)
- Exposure to another person’s suicide or to graphic or sensationalized accounts of suicide
- Previous suicide attempts
- A family history of suicide
- Childhood trauma (e.g., abuse or neglect)
Protective Factors Against Suicide
Carter’s slide described a protective factor as “a characteristic at the individual, family, or community level that is associated with a lower likelihood of suicidal outcomes.” Carter pointed out that protective factors have not been studied as extensively or rigorously as risk factors. “Identifying and understanding protective factors are, however, equally important as researching risk factors,” Carter stated.
Examples of protective factors that Carter listed included:
- Effective clinical care for mental health disorders
- Effective clinical care for substance use disorders
- Effective clinical care for physical health disorders
- Easy access to a variety of clinical interventions
- Ongoing support for medical and mental health care
- Skills in problem-solving, conflict resolution, and nonviolent ways of handling disputes
Carter cautioned her audience, “Multiple risk factors are usually involved. No single risk or protective factor can fully predict or explain suicide. High risk for suicide, whether individuals or communities, usually involves multiple risk factors, as I mentioned before.”
Carter also stressed that context matters: “Although risk factors generally contribute to long-term risk, immediate stressors or painful life experiences may create the final impetus for a suicidal act. Immediate stressors may include relationship problems or a breakup, financial hardship, legal difficulties, public humiliation or shame, a worsening medical prognosis, and other stressful events.”
While a list of risk and protective factors cannot fully predict whether a person will commit a suicidal act or be protected from committing such an act, Carter said, “What it does do is allow us to understand the complexity of issues that make it more likely for someone to die by suicide and also protect individuals from wanting to die by suicide. One thing that we can do to help be an external protective factor is to understand and know the warning signs and figure out what we can do to get them the help they need. This is why a comprehensive approach to suicide is important and necessary.”
Suicide Prevention Strategies, Programs, and Practices to Consider:
Carter averred, “Effective suicide prevention is comprehensive. It requires a combination of efforts that work together to address different aspects of the problem.”
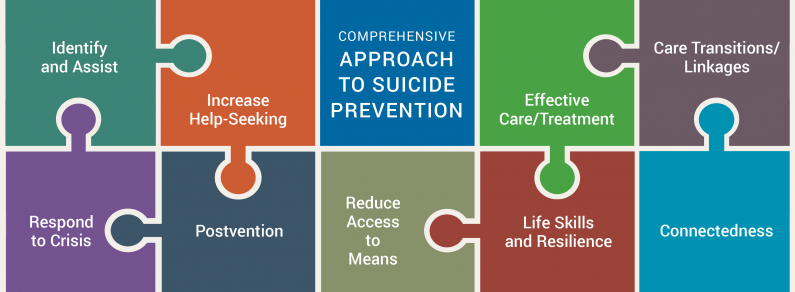
Carter displayed a slide showing a graphic [2] from the Suicide Prevention Resource Center. The graphic depicts several puzzle pieces fitted together. Each puzzle piece represents an element of a comprehensive approach to suicide.
{kind=link}
Referencing the graphic, Carter said, “This model of a comprehensive approach was adapted from a model developed for campuses by the Suicide Prevention Resource Center, or SPRC, and the JED Foundation drawing on the US Air Force Suicide Prevention Program. It shows nine strategies that form a comprehensive approach to suicide prevention and mental health promotion.”
She continued, “Each strategy is a broad goal that can be advanced through an array of possible activities. If we take a look at each of the puzzle pieces that form a comprehensive approach to suicide prevention, we see how they all complement each other.”
Carter discussed each of the nine strategies in turn, offering examples.
Identify and Assist
“We know that many people in distress don’t seek help or support on their own,” Carter said, “Identifying people at risk for suicide can help us reach those in the greatest need and connect them to care and support.”
Examples of methods that can be used to identify those at risk include:
- Appropriate training in identifying those at risk (e.g., QPR Gatekeeper Training, LivingWorks safeTALK, LivingWorks ASIST)
- Screening using an appropriate tool (e.g., Columbia-Suicide Severity Rating Scale [C-SSRS], PHQ-9, or Ask Suicide-Screening Questions [ASQ])
Increase Help-Seeking
- Provide self-help tools.
- Create outreach campaigns to ensure people know what services exist and combat the idea that help might not be effective.
- Address the social and structural environment by fostering peer norms that support help-seeking.
- Make services more convenient and/or more culturally appropriate.
Effective Care/Treatment
Ensure individuals with suicide risks have timely access to evidence-based treatment, suicide prevention interventions, and coordinated systems of care.
Care Transitions/Linkages
Transitions and linkage to care helps ensure people have uninterrupted care during transitions between services and facilitate the exchange of information among the various individuals and organizations providing care to that individual.
Examples of tools and practices that support continuity of care include:
- A formal referral protocol
- Inter-agency agreement
- Cross-training of care providers
- Follow up with the at-risk individual
- Rapid referrals
- Patient and family education.
Respond to Crises
Crisis response should include the full continuum of care. This means not only having hotlines available but also mobile crisis teams, walk-in crisis clinics, hospital-based psychiatry, emergency services, peer support programs, etc.
“Crisis services directly address suicide risk by providing an evaluation, stabilization, and referral to ongoing care,” Carter explained.
Life Skills and Resilience
Life skills such as critical thinking, stress management, and coping can help prepare individuals to safely address challenges they may encounter in their lives, such as financial stress, divorce or other relationship difficulties, physical illness, etc.
Connectedness
Reduce isolation, promote a sense of belonging or community, and foster emotionally supportive relationships. Creating social programs for specific population groups is one way to do this.
Reducing Access to Means
Reducing access to lethal means includes educating families of those in crisis about safety, appropriate medication storage, and safe firearm storage. It can also include activities like distributing gun safety locks, changing medication packaging, and installing barriers on bridges.
Postvention
“Postvention helps organizations or a community respond effectively and compassionately to a suicide death. Postvention is really a part of prevention,” Carter explained.
Identifying Community Readiness to Address Suicide Prevention
“Our good mental health and suicide prevention begin where we live, work, and play,” Carter stated.
Carter explained that the suicide prevention efforts her team has been making are funded by both the state of Minnesota and the federal government. “We have a current Garrett Lee Smith Suicide Prevention Grant which really allowed us to take a comprehensive look into what comprehensive suicide prevention looks like and how we can put it into action in Minnesota,” she explained.
Carter also described how her team decided which communities to target: “When we started to look, we knew that we couldn’t look at the entire state as a whole, so we knew that we needed to take bits and pieces of the state to figure out where there was the biggest need, where there was the capacity to be able to take on the project of comprehensive suicide prevention, and also where communities had readiness. Because not everybody and not every community is ready to talk about what suicide prevention looks like.”
How did they identify community readiness and capacity? Carter explained using a graphic showing “Suicide Prevention” as the center of a stool with three legs supporting it: Need, Capacity, and Readiness.
“Like three legs of the stool, if we identify where there’s need, identify where there is capacity, and identify where there is readiness, we know that our stool will stand up and that we can do some effective suicide prevention,” she explained.
Need
Carter’s team used data to guide their efforts. The data sources they used were:
- Minnesota Student Survey (voluntarily administered in school districts across the state every three years to 5th, 8th, 9th, and 11th grade students)
- Hospital discharge data for self-directed violence
- Demographic data for the state of Minnesota to help identify communities with a significant population of known at-risk individuals (e.g., communities with a higher percentage of American Indian youth)
In the end, the team determined the greatest need was youth ages 10–24, with an emphasis on Minnesota’s American Indian youth population. That became the focus of their project.
Capacity
Carter said, “We looked to build capacity within our organization. The Minnesota Department of Health and Human Services has been working to pilot certified community behavioral health centers. DHS also coordinates mobile crisis stabilization in our state. Our suicide prevention unit team includes a tribal liaison and a coordinator to support our tribal partners to really build that capacity. Our 11 tribal nations in Minnesota, as well as our urban communities, have played a part in this.
“We looked at where there were tribal health clinics and Indian Health Services. We looked at what agencies, schools, and systems had already begun implementing programs as they related to suicide prevention or even prevention efforts in general. We have regional coordinators that are working with school systems, juvenile justice systems, as well as non-profit, business, and community groups. We’re working within each of these systems and groups, assisting them to assess, organizationally, where they are at with comprehensive suicide prevention, planning, and assessing their workforce perceptions of suicide.”
Readiness
“While assessing those partners that had capacity or were building capacity, we looked at building the partnerships where there was a level of readiness,” Carter said. This included:
- Communities that were doing strategic planning and were already engaging in or implementing suicide prevention efforts
- Communities that were reaching out for support
- Communities with existing coalitions focused on suicide prevention work
- Communities that had already begun work on the Community Readiness Model for suicide prevention
- Local public health departments and Statewide Health Improvement Partnership (SHIP) members are looking at mental health as a priority
“As with many initiatives, if there’s leadership buy-in and willingness, there’s a greater chance of success with implementation,” Carter noted.
Comprehensive Healthcare Suicide Prevention: The Zero Suicide Model
The Zero Suicide Model is a comprehensive approach to suicide prevention within healthcare systems with the bold goal of reducing suicides for patients in care to zero. “Attempting to reduce suicides for patients in care to zero may seem scary or even impossible, but what other number should we really strive for?” Carter asked.
The Zero Suicide Model is based on the idea that suicides for people under care are preventable. This approach aims to improve care and outcomes for those patients at risk of suicide by emphasizing the need to transform healthcare for those at risk through a focus on safety and error reduction as well as the use of best practices in suicide care.
Carter noted that several health systems that have implemented the Zero Suicide Model have seen significant reductions in suicide among their patient populations, some by as much as 70–80%.
The seven core elements that make the Zero Suicide Model a comprehensive approach are:
- Lead system-wide culture change committed to reducing suicides. “If we don’t have good leadership on board, more than likely our efforts aren’t going to move forward,” Carter said.
- Train and develop a confident, competent, and caring workforce.
- Identify every person at risk for suicide using standardized, evidence-based tools.
- Engage those at risk for suicide to collaborate in a suicide care management plan.
- Treat suicidal thoughts and behaviors using evidence-based treatment that directly targets suicidality.
- Provide transition services by providing continuous contact and support for those at risk, especially during discharge from acute care settings.
- Improve efforts by applying data-driven quality improvement
Comprehensive School Suicide Prevention
Carter noted that the Zero Suicide model is really designed for health and behavioral healthcare systems but that similar models can be used in other areas of the community, such as schools.
Carter explained how her team engaged with schools in an assessment process and helped them establish a core team or use an existing team to spearhead suicide prevention efforts, using a similar model to the Zero Suicide Model.
Carter said her team makes recommendations based on the Minnesota Student Survey data within their school as well as interviews conducted with the school staff and leadership. Then, her team supports the development of a work plan and provides training and technical assistance as needed. They meet with the school team regularly.
Comprehensive Community Suicide Prevention
When working with communities to implement comprehensive suicide prevention, Carter’s team uses the Community Readiness Model. “We’re specifically looking at the issue of suicide within the community. The model is a starting point for communities to begin suicide prevention work, matching intervention with the level of readiness to achieve the most success. It is a guide that communities can use that builds cooperation and is community-driven,” Carter explained.
The Community Readiness Model assesses six Dimensions Of Readiness: [3]
- Community efforts
- Knowledge of efforts
- Leadership
- Community Climate
- Community knowledge about the issue
- Resources
The process involved identifying community stakeholders who are interviewed with a set of established questions that assess each of these dimensions. The model also includes a process for scoring the dimensions with a readiness score.
Conclusion
Carter shared a quote that inspires her, most popularly attributed to 20th-century anthropologist Margaret Mead: “Never doubt that a small group of thoughtful, committed citizens can change the world; indeed, it’s the only thing that ever has.”
She encouraged her audience: “So, as we look and move further into comprehensive suicide prevention across Minnesota, I really believe that we can all make a difference.”
References
- 988 Suicide & Crisis Lifeline. “988 Suicide and Crisis Lifeline.” Federal Communications Commission, (n.d.), https://www.fcc.gov/988-suicide-and-crisis-lifeline. Accessed May 30, 2024.
- Suicide Prevention Resource Center. Puzzle Complete. A series of puzzle pieces laid out in a 2×5 grid depicts elements of a comprehensive approach to suicide prevention. March 2023. SPRC.org, https://sprc.org/effective-prevention/comprehensive-approach. Accessed May 31, 2024.
- Tri-Ethnic Center for Prevention Research, Colorado State University, et al. Community Readiness: A Handbook for Successful Change. A model that assesses a community’s readiness for change. 2014. SPRC.org, https://sprc.org/online-library/community-readiness-for-community-change/. Accessed May 31, 2024.